

Progress in medicine this week: a breakthrough cardiac drug, a new cancer drug, and more...

Welcome! Lots happened this week, let’s get into it.
1. A breakthrough cardiac drug
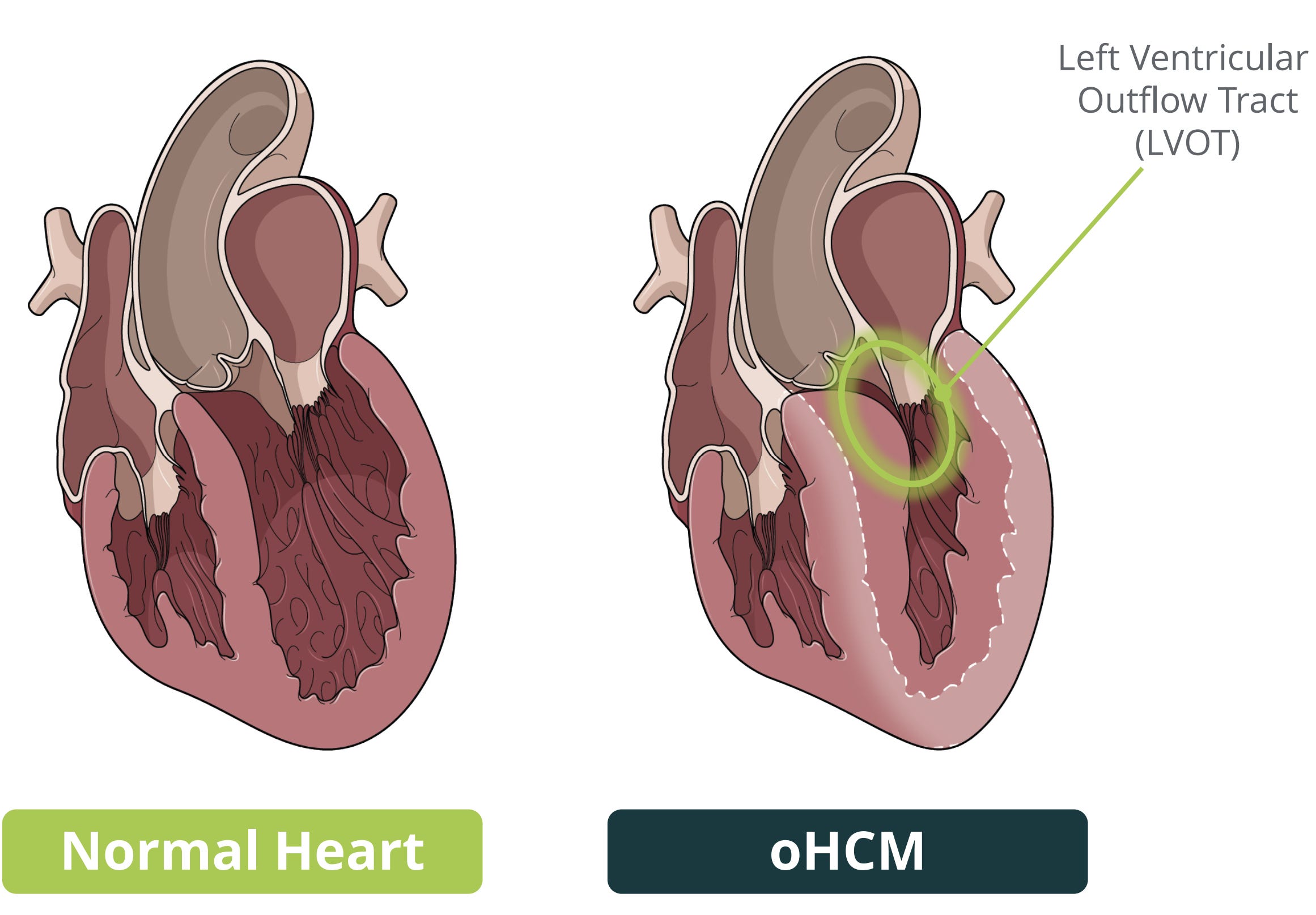
The most common genetic heart condition is hypertrophic cardiomyopathy — it affects about 1:200-500 people (though not all of these manifest symptoms). It causes thickening of the left side of the heart, due to a range of mutations — most commonly, in the proteins that help heart muscle contraction, like myosin.
This hypertrophy can obstruct the ejection of blood from the heart (via the left ventricular outflow tract), which happens in 50-70% of diagnosed patients:
There are two drugs approved to help here — Bristol Myers Squibbs’ Mavacamten and Cytokinetics’ Aficamten. They work in the same way: inhibition of cardiac myosin, which means the heart muscle contracts less forcefully and the obstruction is relieved.
The major unmet need remains the 30-50% of patients with non-obstructive disease, where there are no disease-modifying therapies, but there’s still a risk of heart failure, arrhythmias, and sudden cardiac death.
Bristol’s trial with Mavacamten, which read out last year, was negative for this indication (below, left). This week, Cytokinetics read out a similar trial with Aficamten, which was resoundingly positive (below, right):
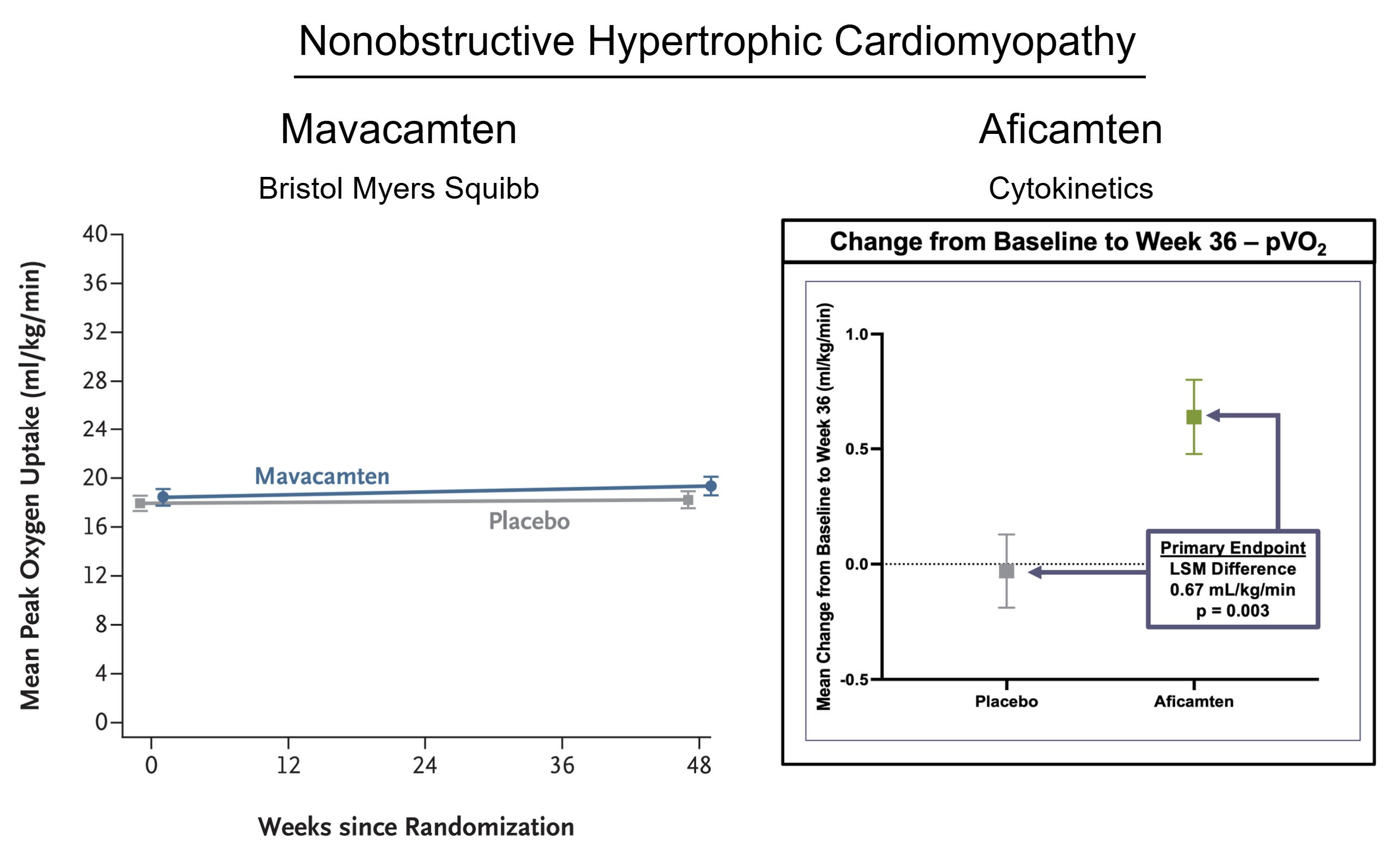
The primary outcome here is peak VO₂, which is basically a measure of exercise capacity. The other readout is ‘KCCQ-CSS’, which measures symptom burden and physical limitation — Aficamten was positive there too (Mavacamten was negative).
If approved, Aficamten will become the first drug specifically approved for non-obstructive hypertrophic cardiomyopathy, which affects about 5–12 million people globally.
2. The first published clinical Daraxonrasib data
This year’s breakthrough of the year is likely to go to Daraxonrasib, which recently read out a positive phase 3 trial in 2nd line metastatic pancreatic cancer, and a positive phase 1/2 in the 1st line. But this week the first clinical data were published (in the NEJM — where else?).
Daraxonrasib targets RAS, the most commonly-mutated oncogene in cancer — it’s a driver in ~90% of pancreas cancers, ~30% of lung adenocarcinomas, and ~40% of colorectal cancers.
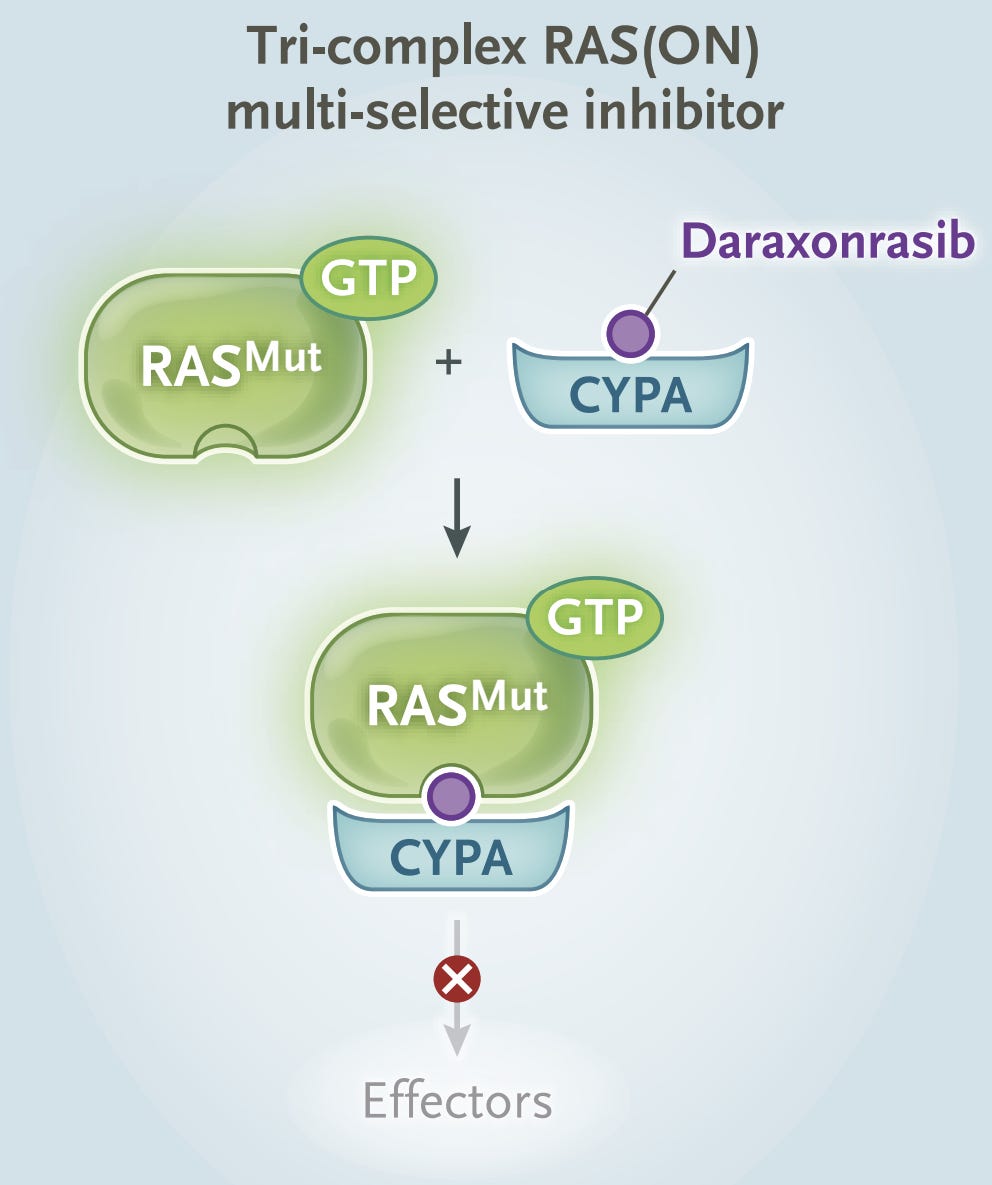
Daraxonrasib is a molecular glue which binds to a scaffolding protein (called Cyclophilin A) and then RAS. This trimer locks RAS into an inactive state that’s unable to activate the downstream pathway, and promotes GTP hydrolysis — to push RAS into the ‘off’ state.
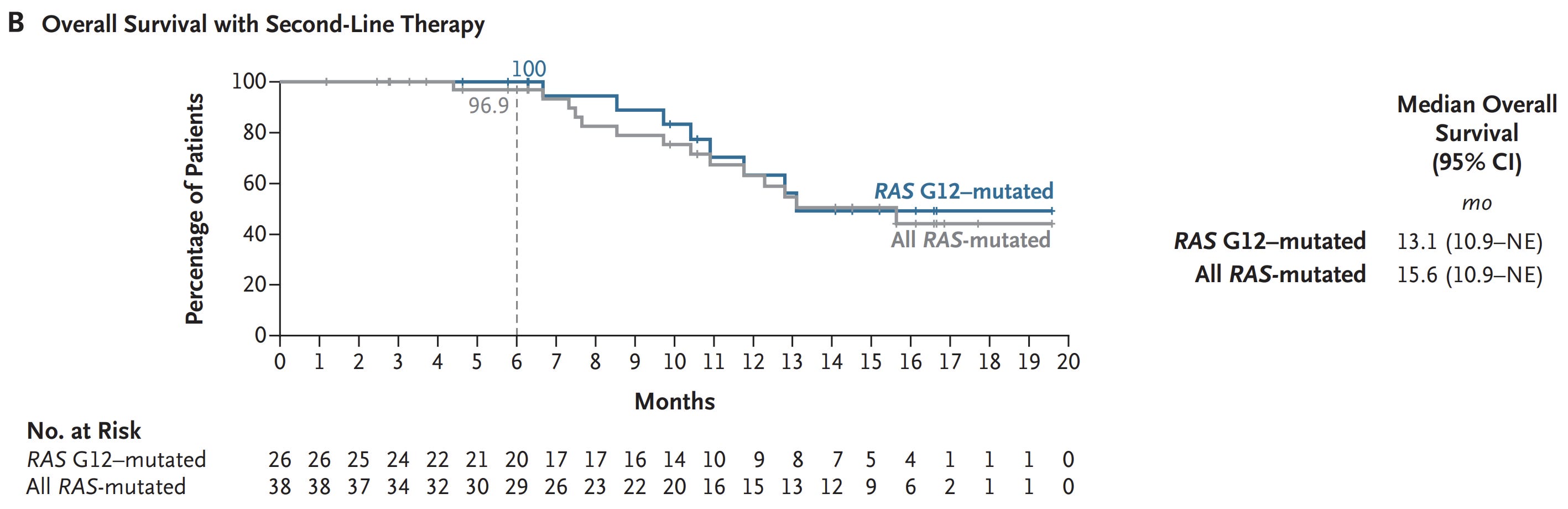
The published data are from a phase 1/2 trial in metastatic pancreas cancer. In the 2nd line of therapy, median overall survival was 15.6 months (which roughly matches the press-released top line from the phase 3) — for context, overall survival with standard-of-care chemotherapy in this setting is typically about 5-7 months.
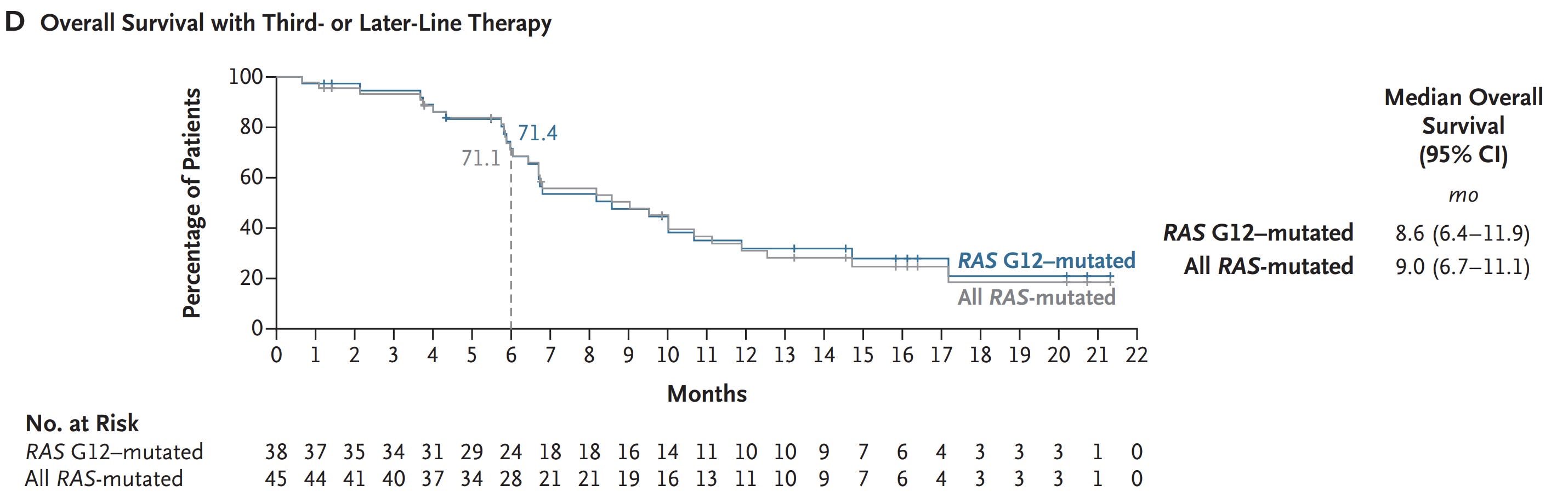
In the 3rd line of therapy, median overall survival was 9.0 months. Overall survival here, with standard-of-care chemotherapy, is about 5.5 months.
What’s next for Daraxonrasib?
The next milestone will be the full presentation and (probably) co-publication of the full randomized 2nd line data in metastatic pancreatic cancer at the end of May at ASCO. After that, regulatory submissions and 2nd line approval later this year. In 2027, we’ll see completion of the non-small-cell lung cancer trial; in 2028, completion of the first-line metastatic pancreatic cancer trial; and in 2030, completion of the adjuvant/resected pancreatic ductal adenocarcinoma trial.
