

This week in medicine: preventing pancreatitis, a new dementia drug target, and more.

Welcome! Every week I analyse the most important things that happened in the world of medicine — papers, trials, approvals. Let’s get into it.
1. The first approved medicine to prevent pancreatitis
I’m fascinated by the idea of new medicines based on genetic evidence. This week another was approved, to prevent pancreatitis. Pancreatitis is severe inflammation of the pancreas. Most patients fully recover, but about 10% need intensive care, and the case fatality is still about 5%.
~10% of cases are caused by high levels of triglycerides, which can clog pancreatic vessels — but this is still not really respected (in my experience) as a serious cause of pancreatitis. This is probably because we don’t have any medicines that can actually prevent pancreatitis in those with severe hypertriglyceridemia — which affects ~1 in 100 people, and carries a ~4-5% annual risk of acute pancreatitis.
People with severe hypertriglyceridemia tend to be those with metabolic syndrome: obesity, diabetes, and liver disease, which disrupts triglyceride metabolism.

The genetic evidence is that people born with loss-of-function APOC3 variants have low triglyceride levels — mechanistically, this is because of increased activity of lipoprotein lipase, an enzyme that breaks down triglycerides.
Based on this, Ionis Pharma developed Olezarsen, an antisense oligonucleotide that reduces triglycerides by silencing the APOC3 mRNA. Olezarsen was just approved this week, based on the trial where it cut the risk of pancreatitis by 85% in those with severe hypertriglyceridemia:

Beyond pancreatitis, high triglycerides also contribute to arterial plaques, so can cause cardiovascular disease: the next question is whether APOC3-targeting therapies can reduce that risk, and those trials (for example, from Arrowhead Pharma) are ongoing.
2. An emerging new mode-of-action to treat ulcerative colitis
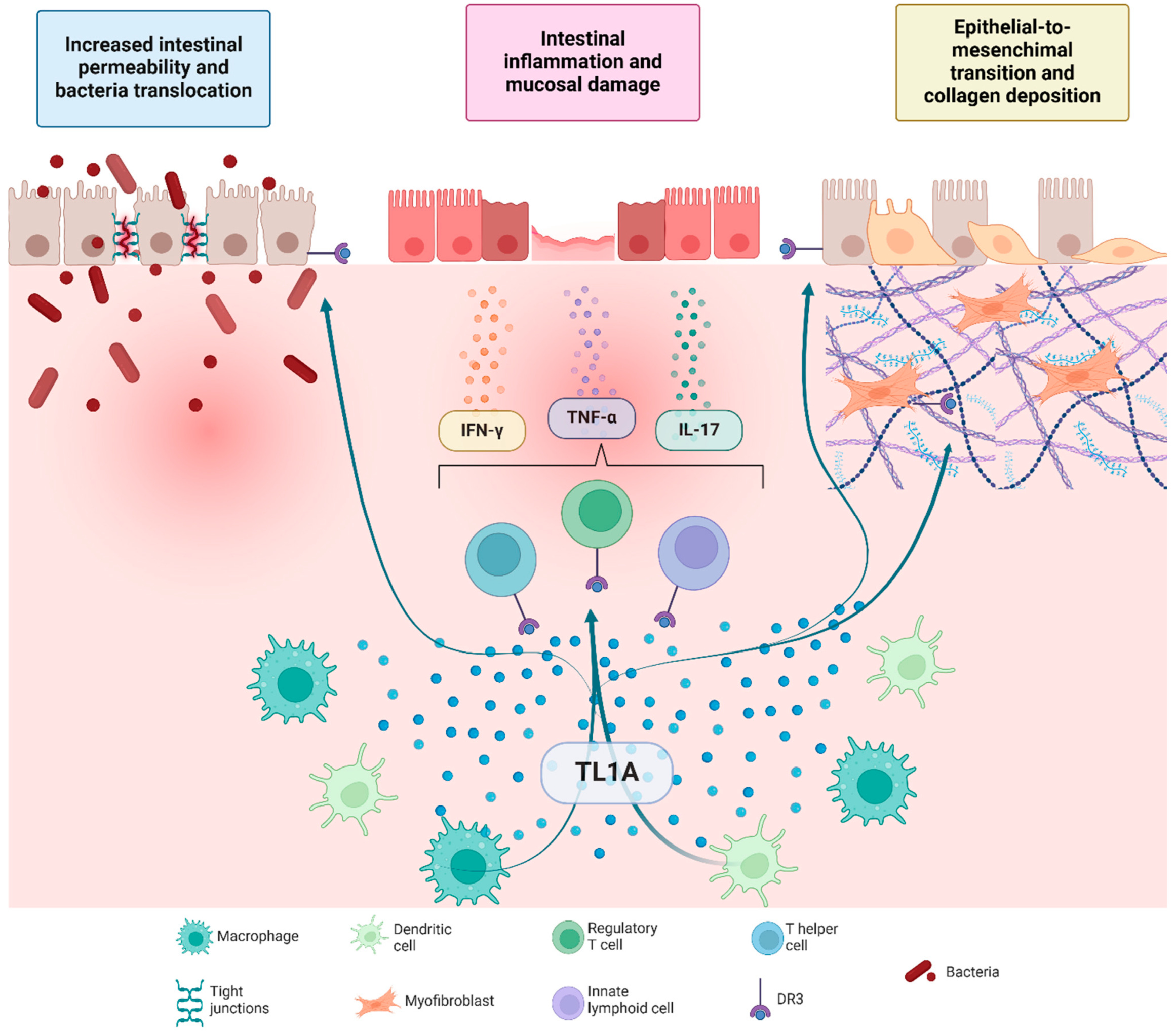
Another emerging target based on genetic evidence is TL1A, the TNF-superfamily ligand, in inflammatory bowel disease (ulcerative colitis and Crohn’s disease). Genetic variants in TL1A increase the risk of ulcerative colitis — it sits upstream of several inflammatory pathways, which means that blocking it might result in remission in a broader range of patients than blocking the individual pathways (like TNF or IL-23).
TL1A also directly activates the fibroblasts that drive fibrosis — so it might be particularly helpful to treat fibrostenotic Crohn’s, where there are still no therapies.
This week, Merck announced positive phase 3 data for their TL1A inhibitor, Tulisokibart, in the induction phase of ulcerative colitis. They’ve said it met the primary endpoint... but haven’t actually told us the numbers.
To see how it looks in context, I put the clinical remission with Tulisokibart — from its previous phase 2 trial — together with its competitors from phase 3. Tulisokibart’s 25% placebo-adjusted remission is not far from best-in-disease, in this cross-trial comparison:
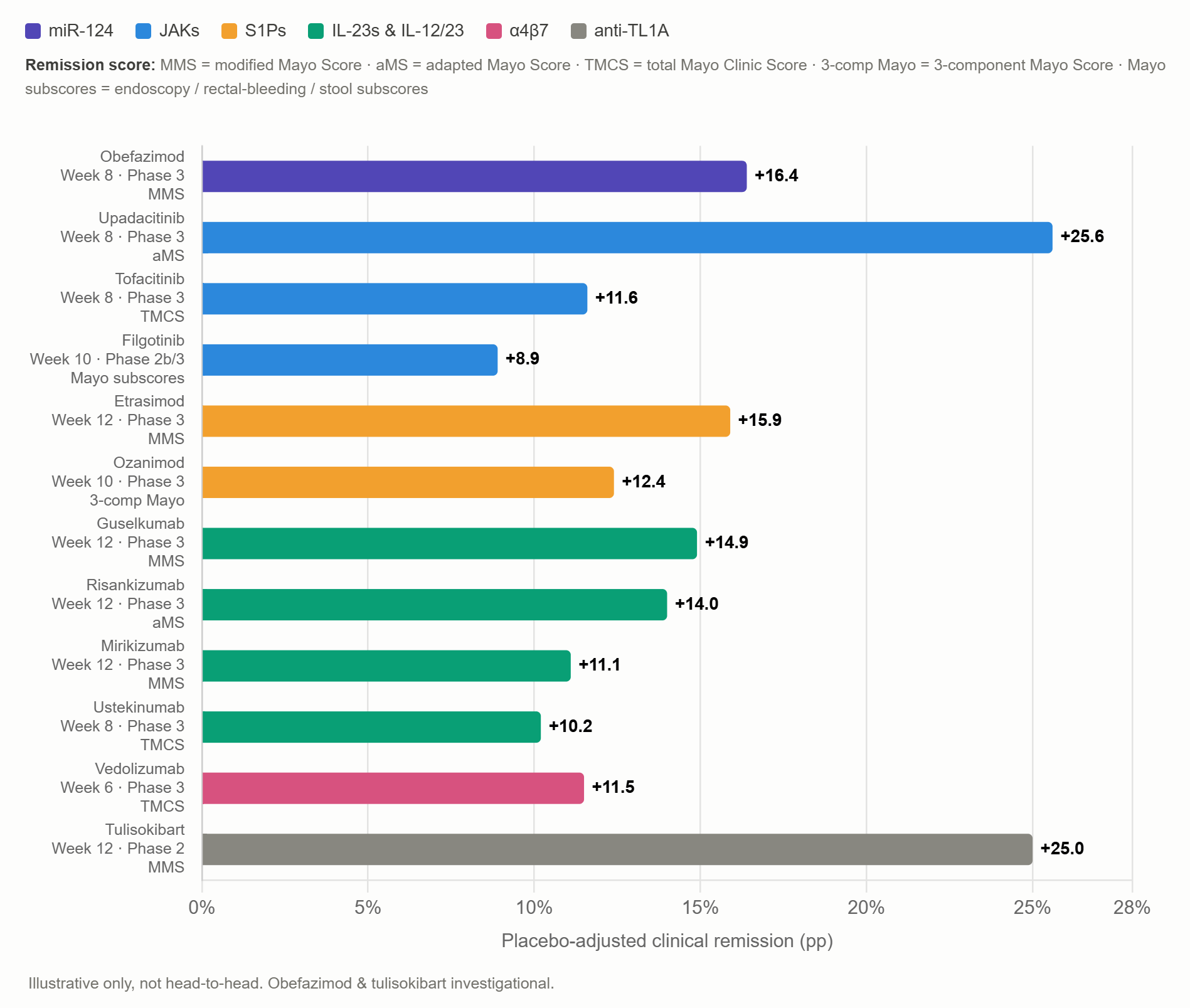
This chart shows that, even with the most effective therapies, most people still do not achieve remission. I spoke to an inflammatory bowel disease specialist about this, who confirmed to me that, to solve this, (at least) two things are needed: 1) more drugs, with differentiated mechanisms-of-action 2) better understanding of disease heterogeneity and subgroups — and better diagnostic tests to pinpoint them — so we can tailor medicines to the right patients.
3. A KRAS G12D inhibitor in pancreatic cancer
Next week is the gastrointestinal cancer conference (ESMO GI) in Munich. I will be there! Arguably the most interesting abstract is from Revolution Medicines, with an inhibitor of KRAS G12D, the most common mutation in pancreatic cancer.
")
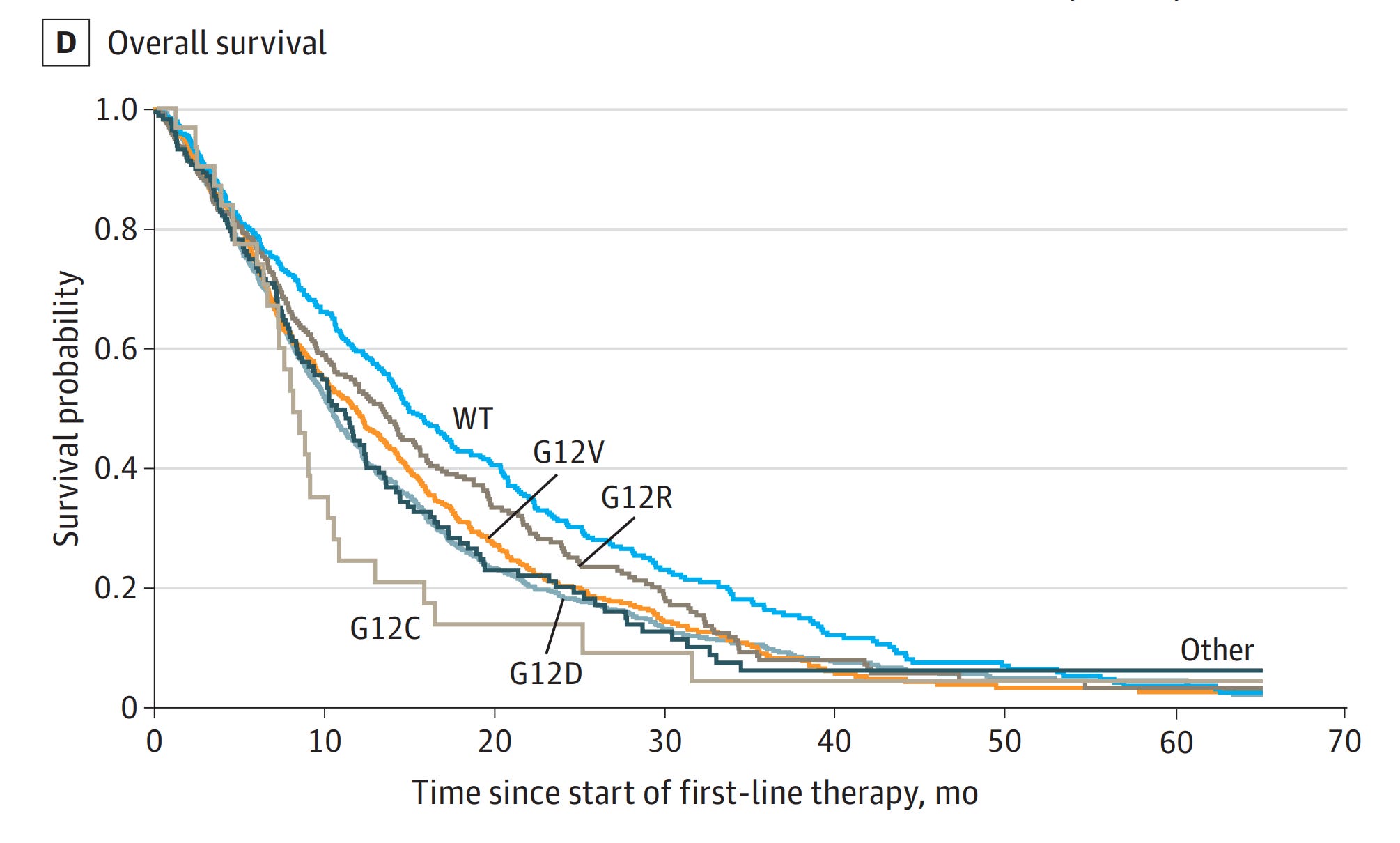
It’s not only the commonest, but the G12D mutation also correlates with worse survival than some of the other KRAS mutants:
The trial tests Zoldonrasib, which works in a similar way to Daraxonrasib. It’s an oral, RAS(ON) tri-complex inhibitor, that uses cyclophilin A to inhibit the active form of KRAS G12D.
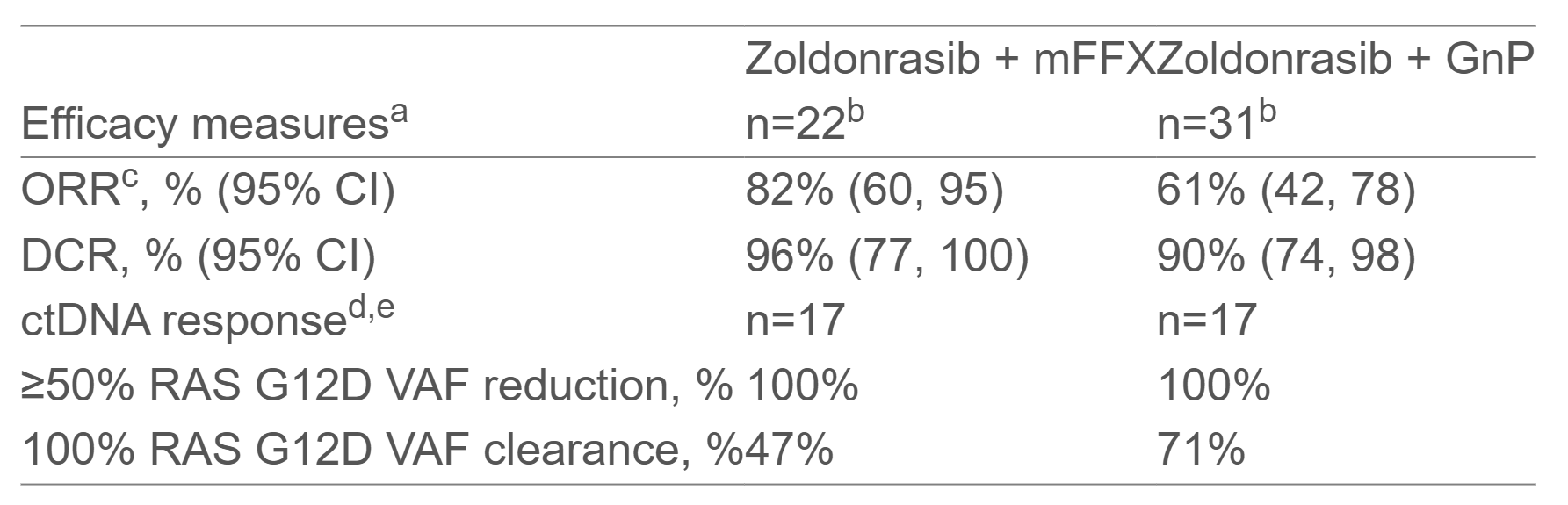
This week, RevMed announced the data from the phase 1/2 trial. Combined with the current standard-of-care chemotherapies, mFOLFIRINOX or Gemcitabine/nab-Paclitaxel (whose objective response rate, ORR, in this setting is ~23-43% and ~32-42%, respectively) addition of Zoldonrasib achieved 82% and 61% ORR, respectively:
It’s notable that grade 3 adverse events (which are severe enough to consider hospitalisation) were above 60% in this trial, though much of this is from the chemotherapy.
One of the potential benefits of using a G12D-specific inhibitor (Zoldonrasib) over a multispecific RAS inhibitor (Daraxonrasib, which also inhibits the wildtype RAS that normal cells express) is reduced toxicity. Indeed, in this trial, incidence of rash was 18% with Zoldonrasib, compared to ~ 90% in previous Daraxonrasib trials.
